Medical treatment for vitiligo isn't always necessary. For some, skin color returns without treatment. For others, self-care steps, such as using sunscreen and applying cosmetic camouflage cream, may improve the appearance of your skin. For fair-skinned individuals, avoiding tanning can make the areas almost unnoticeable.Depending on the number, size and location of the white patches, you may decide to seek medical treatment. Medical treatments for vitiligo aim to even out skin tone, either by restoring color (pigment) or by destroying the remaining color. Treatment for vitiligo may take as long as six to 24 months, and you may have to try more than one treatment before you find the one that works best for you.
Medical therapies
Topical corticosteroid therapy. Corticosteroids may help return color to your skin (repigmentation), particularly if the medication is started early in the disease. Milder topical corticosteroid cream or ointment may be prescribed for children and for people who have large areas of depigmented skin. It may take as long as three months of treatment before you begin to see any changes in your skin's color. This treatment is easy and effective, but your doctor needs to monitor you closely for side effects, such as thinning of the skin (atrophy) and streaks or lines on your skin (skin striae). Calcipotriene (Dovonex), a vitamin D derivative, also may be used topically and is sometimes used with corticosteroids or ultraviolet light.
Topical immunomodulators. Topical ointments containing tacrolimus or pimecrolimus are effective for people. This treatment may have fewer side effects than corticosteroids and can be used in combination with ultraviolet B (UVB) treatments.
Topical psoralen plus ultraviolet A (PUVA). This option, which is also called photochemotherapy, may be effective for you if less than 20 percent of your body has depigmented patches. You'll have to visit the doctor once or twice a week for treatment. Your doctor or nurse applies a thin coating of the topical psoralen about 30 minutes before the light exposure. Psoralen makes your skin more sensitive to ultraviolet light. Your skin is then exposed to UVA light, which turns the treated areas pink. As the skin heals, a more normal skin color appears.
A variation is known as water bath PUVA, in which you lie in a tub of water containing psoralen for 15 minutes before you're exposed to the light.
Possible side effects include severe sunburn and blistering, though you can minimize your risk of complications by avoiding direct sunlight after each treatment. Hyperpigmentation — overdarkening of the skin — is usually temporary and eventually lightens when treatment stops.
Oral psoralen photochemotherapy (oral PUVA). If you have depigmented areas that cover more than 20 percent of your body, your doctor may recommend oral psoralen. For this treatment, you take the oral psoralen about two hours before exposure to UVA light. You'll have to visit the doctor two or three times a week, allowing for at least a day in between treatments. As with topical psoralen, the treated skin becomes pink after UVA exposure, and then eventually fades to a more normal skin tone.
This treatment can also be done using natural sunlight if you don't have access to a doctor's office with the proper equipment. Your doctor will let you know how much exposure you need and will want to monitor your skin changes frequently.
Sunburn, nausea, vomiting, itching, abnormal hair growth and overdarkening of the skin are potential short-term side effects of this treatment, whether it's done in the doctor's office or using natural sun. Your risk of skin cancer may be increased if you use this therapy long term. Oral PUVA is not recommended for children under 10 due to a greater risk of damage to the eyes, such as cataracts.
You can reduce your odds of skin cancer and sunburn by staying out of direct sunlight for one to two full days after treatment. The use of sunscreen can also help reduce your risk of side effects. To protect your eyes from serious damage, such as cataracts, wear UV-protective sunglasses for up to 24 hours after each treatment when you're exposed to the sun.
Narrowband ultraviolet B (UVB) therapy. Narrowband UVB, a special form of UVB light that uses a more specific wavelength of ultraviolet B, is an alternative to PUVA. This type of therapy can be administered like PUVA and given up to three times a week. However, no pre-application of psoralen is required, which simplifies the treatment process. Because it is simpler to administer, this type of phototherapy is gaining wide acceptance. However, more research is needed to determine if it is superior to PUVA and to assess its long-term safety. Narrowband wavelengths of light can also be delivered to smaller areas of vitiligo using either an intense light source (focal) or a laser. Small trials have shown positive results. However, due to the added expense of these devices they may not be available in all dermatologists' offices.
Excimer laser. This type of laser delivers controlled beams of a specific wavelength of UVB light to the skin. It can be used only on small areas of vitiligo, and it's often used in combination with topical drugs. Side effects can include redness and blistering.
Depigmentation. Depigmentation may be an option for you if you have vitiligo that covers more than half of your skin. Depigmentation therapy lightens the unaffected parts of your skin to match the areas that have already lost color. For this treatment, you apply a medication called monobenzone ether of hydroquinone twice a day to the areas of your skin that still have pigment. Treatment continues until the darker areas of your skin match the already-depigmented areas.
Redness and swelling are potential side effects of depigmentation therapy, and you have to be careful to avoid skin-to-skin contact with other people for at least two hours after you've applied the drug, so you don't transfer it to them. Other potential side effects include itching and dry skin. Depigmentation is permanent and will make you extremely sensitive to sunlight permanently.
Autologous skin grafts. This type of skin grafting uses your own tissues (autologous). Your doctor removes tiny pieces of skin from one area of your body and attaches them to another. This procedure is sometimes used if you have small patches of vitiligo. Your doctor removes very small sections of your normal, pigmented skin, often containing a small hair, and places them on areas that have lost pigment. Possible complications include scarring, a cobblestone appearance, spotty pigmentation or failure of the transferred skin to repigment.
Blister grafting. In this procedure, your doctor creates blisters on your pigmented skin, primarily by using suction. The tops of the blisters are removed and transplanted where a blister of equal size has been created and removed in an area that has no pigment. Blister grafting may cause a cobblestone appearance and scarring, and the area may not repigment. However, there's less risk of scarring with this procedure than with other types of skin grafting.
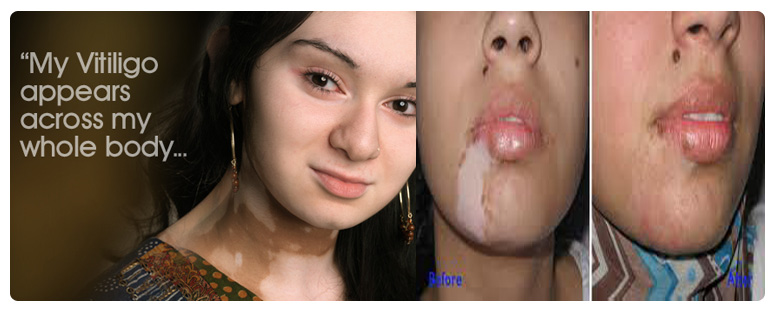
Tattooing (micropigmentation). Tattooing implants pigment into your skin with a special surgical instrument. For the treatment of vitiligo, tattooing is most effective around the lips and in people with dark skin. Sometimes the tattoo color doesn't match skin color closely enough. Additionally, tattoo colors fade and they don't tan.
Experimental Therapies
Doctors are continuing to try to find better ways to treat vitiligo. One newer option is a procedure called an autologous melanocyte transplant. Using a sample of your normal skin, researchers can grow melanocytes in the lab. These newly developed melanocytes are then transplanted to the areas on your body that lack pigment. This treatment is still considered experimental and isn't widely available.
Another treatment in development uses a compound found in black pepper called piperine. In trials on mice, piperine was found to be effective at causing repigmentation. Piperine was even more effective when it was used in combination with UV light. Redness and skin peeling were temporary side effects of this treatment.
Make an Appointment
call now : 091533 19842 / 072787 51087 (Prasenjit Das, Assistant)
Columbia Asia Hospital
IB 193, Sector - III, Salt Lake City,
Kolkata - 700 091, West Bengal, India
Phone : 033 3989 8969 Fax : 033 2335 7078
Harlem Point
56, J. L. Nehru Road,
Kolkata - 700 020, West Bengal, India
Tel : 033 2282 3573 / 033 4003 4006
Monday, Wednesday, Saturday: 3.00 - 5.00 p.m
North City Hospital
Opp. Hudco, Ultadanga
Kolkata - , West Bengal, India
Tel : 033 2321 1101 / 02
Friday : 4 - 6 p.m.