| Treatment |
| |
|
| HIGH RISK PREGNANCY : |
| |
| I have a high-risk pregnancy. What does that mean? |
| |
If your pregnancy is high-risk, it means you need extra care to help you have a healthy pregnancy and baby. If you're being treated for a lifelong (chronic) condition, you may have known for a long time that becoming pregnant carries additional risks. Or you may find out you have a high-risk pregnancy because of a problem that develops for the first time during pregnancy.
Either way, having a high-risk pregnancy means it's more likely that you or your baby will have health problems during pregnancy, birth, or after delivery. These could be very minor problems, but in some cases, a high-risk condition can be life threatening for a woman or her baby. That's why a high-risk pregnancy requires extra monitoring by a healthcare provider. |
|
 |
| |
 |
|
Being told that your pregnancy is high-risk can be a shock, and you're likely to feel a mix of emotions. You might find it difficult to enjoy your pregnancy because you're worried about your own health or your baby's health.
Ask your provider for information about your pregnancy and how to prevent or manage problems. Building a support network, talking to your partner, family and friends, or other women in a similar situation, can help you feel better informed and more in control.
It's likely you'll hear and read about many issues and complications that could affect your pregnancy. But having a high-risk pregnancy doesn't mean you won't have a healthy baby. So don't give up hope. |
|
| |
| |
| What causes a high-risk pregnancy? |
|
 |
| |
| Many factors can make a pregnancy high-risk. |
| |
You may be considered high risk if you had problems in a previous pregnancy – if you delivered a baby early, for example. This doesn't mean you'll definitely experience the same problems again, but your provider will want to keep a closer eye on you as your pregnancy progresses.
Some health conditions can make your pregnancy high-risk too. See a doctor before you start trying to get pregnant if you have a chronic condition, so you can be as healthy as possible before you conceive. There are many health conditions that affect pregnancy including : |
| |
 |
|
● Blood disorders. If you have a blood disorder, such as sickle cell disease or thalassemia, the additional strain pregnancy puts on your body can make your condition worse. There are also potential risks to your baby (both during pregnancy and after delivery) if she inherits your condition.
● Chronic kidney disease. This condition increases your risk of miscarriage, developing high blood pressure and preeclampsia, and having your baby early. Pregnancy can also put an extra strain on your kidneys.
● Depression. Pregnancy and becoming a mom can make you more vulnerable to mental health problems, including anxiety and depression. Untreated depression and some medications for depression are linked with risks for your baby. (However, don't make changes to your medication without talking to your healthcare provider first. Stopping suddenly has risks too.) |
|
| |
● High blood pressure. You can still have a normal pregnancy, even if you have high blood pressure. However, untreated high blood pressure can cause your baby to grow more slowly than usual or be born early. Other complications associated with high blood pressure include preeclampsia and placental abruption, a serious condition in which the placenta partially or completely separates from the uterus before a baby is born.
● HIV or AIDS. If you have HIV or AIDS, your baby can become infected before birth, during delivery, or when you breastfeed. Fortunately, medication can dramatically reduce this risk.
● Lupus. Lupus and other autoimmune diseases can increase your risk of preterm delivery, preeclampsia, and having a small baby. Being pregnant may also increase the likelihood of your disease flaring up or getting worse. |
|
 |
| |
 |
|
● Maternal age. Your age can affect how likely you are to have a high-risk pregnancy. Being an older mom (age 35 or older in your first pregnancy) or a younger one (in your teens) puts you at greater risk of some complications and health problems.
● Obesity. Having a body mass index (BMI) of 30 or higher before pregnancy puts you at greater risk of gestational diabetes, type 2 diabetes, and high blood pressure during your pregnancy. When it comes to giving birth, you're more likely to need your labor induced or a cesarean delivery.
● Thyroid disease. Both an underactive thyroid (hypothyroidism) and an overactive thyroid (hyperthyroidism) during pregnancy can cause problems for you and your baby if the condition isn't controlled. These problems can include miscarriage, preeclampsia, low birth weight, and having your baby early. |
|
| |
| How does being high risk affect my care? |
|
 |
| |
If you have a high-risk pregnancy, you may need more frequent prenatal appointments and will be monitored closely by your providers. You may also be referred to a maternal-fetal medicine (MFM) doctor. This is a physician who is specially trained to care for women who have a high-risk pregnancy.
The exact care you and your baby need depends on your particular circumstances and on the reasons your pregnancy is high-risk. You might see your MFM doctor just once or regularly throughout your pregnancy. Your MFM doctor will work with your ob-gyn and other providers to keep you and your baby healthy as your pregnancy progresses. |
| |
| Will my baby be okay if I'm high-risk? |
| |
 |
|
If you have a high-risk pregnancy, one of your biggest worries will probably be whether any harm will come to your baby. It's natural to be concerned.
However, with good prenatal care it's possible to have a healthy baby. Healthy moms grow healthy babies: That's why it's so important to talk to your provider to find out how best to keep you and your baby safe.
Some conditions, as well as the drugs that are usually prescribed to manage them, pose a risk to your baby's health. But stopping medications that you take for a condition can also be very dangerous. |
|
| |
You may be asked to change the drugs you take for a health condition, such as high blood pressure, to another medication that's safer during pregnancy. This can help to reduce the risk of problems that the side effects of your medication might cause for your baby while he's developing in the uterus. Note: Don't stop taking any medication without consulting your provider first.
If your baby is born early, he could have difficulty breathing or feeding, or develop infections or other complications. If this happens, he needs extra care and support, which means staying in the hospital for several weeks, probably in a neonatal intensive care unit (NICU). |
| |
|
| |
| INFERTILITY SOLUTIONS : |
| |
| What is Infertility? |
|
 |
| |
| Infertility means a couple is not able to become pregnant after 1 year of having regular, unprotected sex. Infertility affects both women and men. A woman is considered infertile if she has tried for 1 year to get pregnant and hasn’t used birth control. A man is considered infertile if he has too few sperm or his sperm are too unhealthy to combine with a woman’s egg. Many couples do not have trouble becoming pregnant. But there are factors that can make it difficult for some. |
| |
| Symptoms of infertility |
| |
The main symptom of infertility is not being able to get pregnant. There may be no other symptoms. For women, if there are symptoms, they are usually related to the cause of infertility.
Certain factors may interfere with getting pregnant. However, these factors do not guarantee you will be infertile. For women, those factors can include:
 Painful or irregular periods (menstrual cycle) Painful or irregular periods (menstrual cycle)- Age (older than 35)
- Endometriosis or pelvic inflammatory disease (diseases of a woman’s reproductive organs)
- Cancer treatment
For men, factors include:
- Infections
- A low sperm count (a higher count increases the chance the sperm and egg will meet)
- Problems with your male reproductive organs (such as undescended testicles, enlarged prostate, and varicoceles, or enlarged veins in the skin that surround a man’s testicles)
- Cancer treatment
Your doctor may recommend you be tested for infertility if any of these factors are concerns. |
| |
| What causes infertility? |
| |
Making a baby (getting pregnant) is complex. Multiple things have to go right for both the man and the woman. Therefore, there are many causes of infertility in women and men.
A woman’s fertility can be affected by:
- This is the process by which the egg leaves the ovary and travels to meet the sperm. Some women don’t ovulate every month, which makes it harder to become pregnant.
- Problems with your reproductive system (fallopian tubes, cervix, uterus, ovaries). This might include a blockage, cancerous or noncancerous growths, scarring, enlarged ovaries, or an abnormal opening of the cervix.
- Disease and disorders. This might include endometriosis (when uterine tissue grows outside the uterus) or polycystic ovary syndrome (having enlarged ovaries containing fluid-filled sacs).
- Early-onset menopause. This would occur before the age of 40. It may be tied to an immune system disease, cancer treatments, or a genetic syndrome.
- As a woman gets older, it becomes harder to get pregnant.
- Cancer treatments. Radiation and chemotherapy affect fertility.
- Smoking and substance abuse. Smoking, alcohol, and drug use can make it difficult to get pregnant.
- Medicines, especially those treating cancer, fungus, and ulcers.
- Being overweight or underweight can affect fertility. Even too much or too little exercise can affect a woman’s chances of getting pregnant.
- Delayed puberty or absence of a period (menstruation).
- Uncontrolled diabetes, autoimmune diseases (when your body attacks itself), lupus, and celiac disease can make it difficult for a woman to become pregnant
A man’s fertility can be affected by:
- Unhealthy or poorly functioning sperm. This includes the quality of the man’s sperm. It also includes how well and how quickly the sperm move as they travel to meet the egg.
- A varicocele — enlarged veins inside the loose skin that surrounds a man’s testicles. It can cause low sperm count.
- This can be a bacterial infection inside the man’s testicles. It can also be a sexually transmitted infection (STI).
- Retrograde ejaculation — a man’s sperm goes into his bladder rather than outside the penis as it is supposed to.
- Autoimmune disorders (when the body attacks itself).
- Cancerous or non-cancerous growths.
- Undescended testicles. One or both of a man’s testicles remain in his abdomen. Testicles are supposed to drop down from the abdomen into the scrotal sac at birth.
 Hormone imbalance. Hormone imbalance.- Blockages within the many tubes that carry a man’s sperm.
- Certain genetic syndromes, such as Down syndrome.
- Medicines, especially those treating cancer, fungus, and ulcers.
- Certain surgeries, including vasectomy (a procedure to prevent sperm from leaving the testicles).
- Smoking and alcohol or drug use.
- Exposure to industrial chemicals and heavy metals.
- Radiation and X-rays.
- Overheating the testicles. This can occur by wearing underwear or pants that are too tight. It can also happen by using a hot tub for extended periods.
Sexual dysfunction — inability to have an erection for sex or problems ejaculating into the vagina (too soon or not at all). This could be due to physical or emotional issues. |
| |
| How is infertility diagnosed? |
| |
For both men and women, your doctor will conduct a routine medical exam. He or she will ask you questions about your general health and how long you have been trying to have a baby. Your doctor will decide what additional testing is necessary.
Additional testing would likely begin with blood tests. These will check hormone levels and genetics (for both men and women) and egg quality. Women may have additional tests. These could include:
- Transvaginal ultrasound. A medical technician will insert a small wand, covered with latex, into your vagina. The wand is connected to a screen, where the technician can view images of the inside of your uterus and fallopian tubes. The technician will send the images to your doctor to review.
- This is an X-ray that involves injecting dye into your uterus to look for blockages inside your fallopian tubes. It does not require anesthesia.
- This surgical procedure is performed in a hospital. A thin, flexible scope is inserted into your abdomen to give your doctor a better look at your uterus and fallopian tubes. It helps look for polyps, growths, and blockages.
For men, the first test will be to collect a sample of his semen (the fluid that is ejaculated from the penis). This is used to examine his sperm count, quality, and movement.
 Men may undergo further physical exams, which would look for: Men may undergo further physical exams, which would look for:
- Past injury to his testicles or penis.
- Discharge (fluid that should not be present in the man’s penis).
- A swollen or enlarged prostate.
- A varicocele (enlarged veins inside the skin around a man’s testicles).
- Recent high fevers.
- A history of mumps.
A biopsy of the man’s testicles may be necessary to get a better sperm sample. |
| |
|
| |
| |
| OVARIAN CYST |
|
 |
| |
| What are ovarian cysts? |
| |
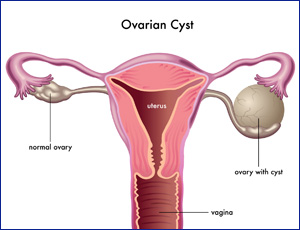
The ovaries are part of the female reproductive system. They’re located in the lower abdomen on both sides of the uterus. Women have two ovaries that produce eggs as well as the hormones estrogen and progesterone.
Sometimes, a fluid-filled sac called a cyst will develop on one of the ovaries. Many women will develop at least one cyst during their lifetime. In most cases, cysts are painless and cause no symptoms. |
| |
| Types of ovarian cysts |
| |
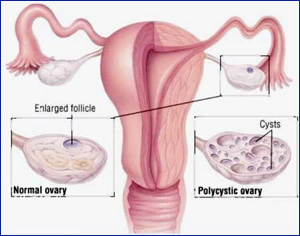
| There are various types of ovarian cysts, such as dermoid cysts and endometrioma cysts. However, functional cysts are the most common type. The two types of functional cysts include follicle and corpus luteum cysts. |
| |
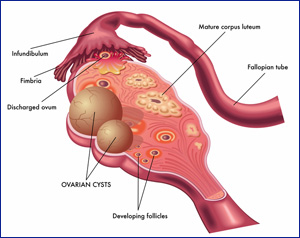
Follicle cyst
During a woman’s menstrual cycle, an egg grows in a sac called a follicle. This sac is located inside the ovaries. In most cases, this follicle or sac breaks open and releases an egg. But if the follicle doesn’t break open, the fluid inside the follicle can form a cyst on the ovary.
Corpus luteum cysts
Follicle sacs typically dissolve after releasing an egg. But if the sac doesn’t dissolve and the opening of the follicle seals, additional fluid can develop inside the sac, and this accumulation of fluid causes a corpus luteum cyst. |
| |
 |
|
Other types of ovarian cysts include:
- dermoid cysts: sac-like growths on the ovaries that can contain hair, fat, and other tissue
- cystadenomas: noncancerous growths that can develop on the outer surface of the ovaries
- endometriomas: tissues that normally grow inside the uterus can develop outside the uterus and attach to the ovaries, resulting in a cyst
Some women develop a condition called polycystic ovary syndrome. This condition means the ovaries contain a large number of small cysts. It can cause the ovaries to enlarge. If left untreated, polycystic ovaries can cause infertility. |
|
| |
| Symptoms of an ovarian cyst |
| |
Often times, ovarian cysts do not cause any symptoms. However, symptoms can appear as the cyst grows. Symptoms may include:
- abdominal bloating or swelling
- painful bowel movements
 pelvic pain before or during the menstrual cycle pelvic pain before or during the menstrual cycle- painful intercourse
- pain in the lower back or thighs
- breast tenderness
- nausea and vomiting
Severe symptoms of an ovarian cyst that require immediate medical attention include:
- severe or sharp pelvic pain
- fever
- faintness or dizziness
- rapid breathing
These symptoms can indicate a ruptured cyst or an ovarian torsion. Both complications can have serious consequences if not treated early. |
| |
| Treatment for an ovarian cyst |
| |
 |
|
Your doctor may recommend treatment to shrink or remove the cyst if it doesn’t go away on its own or if it grows larger.
Birth control pills
If you have recurrent ovarian cysts, your doctor can prescribe oral contraceptives to stop ovulation and prevent the development of new cysts. Oral contraceptives can also reduce your risk of ovarian cancer. The risk of ovarian cancer is higher in postmenopausal women.
Laparoscopy
If your cyst is small and results from an imaging test to rule out cancer, your doctor can perform a laparoscopy to surgically remove the cyst. The procedure involves your doctor making a tiny incision near your navel and then inserting a small instrument into your abdomen to remove the cyst. |
|
| |
| Laparotomy
If you have a large cyst, your doctor can surgically remove the cyst through a large incision in your abdomen. They’ll conduct an immediate biopsy, and if they determine that the cyst is cancerous, they may perform a hysterectomy to remove your ovaries and uterus. |
| |
| Ovarian cyst prevention |
| |
Ovarian cysts can’t be prevented. However, routine gynecologic examinations can detect ovarian cysts early. Benign ovarian cysts don’t become cancerous. However, symptoms of ovarian cancer can mimic symptoms of an ovarian cyst. Thus, it’s important to visit your doctor and receive a correct diagnosis. Alert your doctor to symptoms that may indicate a problem, such as:
- changes in your menstrual cycle
- ongoing pelvic pain
- loss of appetite
- unexplained weight loss
- abdominal fullness
|
| |
|
| PREGNANCY COUNSELING |
| |
The PC Program provides counseling to women who need assistance with decision-making and the emotional stress of an unplanned pregnancy. The infant’s needs are also of utmost importance. We also provide services to the baby’s father and the parents’ families, when appropriate and when not in conflict with the client’s wishes.
Pregnancy Counseling services are available to expectant or newly parenting single or married women. Most clients are single women between 15 and 25 who have never before given birth and who contact the agency in the early to middle of their pregnancy. However, some are older or younger, some are married, divorced or separated. Some have other children. Some contact the agency after delivery. Occasionally a client will bring her baby home for a period of time, then seek counseling about adoption when she feels she cannot parent adequately. |
|
 |
| |
 |
|
Referrals come to the program at any stage of the pregnancy from other CFS programs, prenatal clinics, crisis pregnancy centers, doctors, hospitals, schools, attorneys, family members, or therapists. PC staff collaborates with the referral agent to provide comprehensive service. Clients can be seen at any of our statewide offices, at their home, their school, at their prenatal appointment, or wherever is most comfortable and convenient for them. There are no fees to clients, but we bill Medicaid or their insurance.
The goal of the PC Program is to assist the client in making a comfortable informed plan for herself and her baby. We provide accurate objective information about all their options and encourage her to make an informed independent decision. We offer her an opportunity to explore all her options in the context of her own life, her goals, relationships, values and available resources. Prevention of future pregnancies is also explored and clients are encouraged to consult with their doctor about their family planning options. |
|
| |
Services are available regardless of the client’s choice, whether she chooses termination, parenting, adoption or other custody arrangement for the baby. The philosophy of the program is that self-determination and un-pressured decision-making promotes a comfortable adjustment to whatever decision is made. When adoptions are planned, this philosophy also promotes legally safe adoptions and stable permanence for children.
Services include immediate, objective, in-depth counseling beyond the “options counseling” offered in other programs. We do not impose a set of values or religious tenets upon our clients and our counseling is provided by a master’s level clinical staff. The program is community based and we work with other providers involved.
Services are available in New Hampshire, south of Lebanon, and in bordering states if the client delivers in New Hampshire and the travel distance is manageable. |
|
 |
| |
| |
|
| I.V.F. |
| |
| WHAT IS IVF? |
|
 |
| |
| Infertility issues have shown a rising trend in recent times and getting a treatment for infertility leaves a couple exhausted. They get confused where to go and whom to ask. Come to us as we offer a wide range of treatment methods and services such as I.U.I, I.V.F., Egg Donation, Irregular Period , Gynecological Problem, Embryo Donation, Pre Cycle Evolution, Stimulation of Ovulation & Cycle Monitoring, Semen Preparation, Sperm Donation, Surrogacy and other such services. IVF is the one of the most used treatment method for infertility and we are best at it. |
| |
| How does IVF work? |
| |
 |
|
IVF stands for in vitro fertilization. It’s one of the more widely known types of assisted reproductive technology (ART). IVF works by using a combination of medicines and surgical procedures to help sperm fertilize an egg, and help the fertilized egg implant in your uterus.
First, you take medication that makes several of your eggs mature and ready for fertilization. Then the doctor takes the eggs out of your body and mixes them with sperm in a lab, to help the sperm fertilize the eggs. Then they put 1 or more fertilized eggs (embryos) directly into your uterus. Pregnancy happens if any of the embryos implant in the lining of your uterus.
IVF has many steps, and it takes several months to complete the whole process. It sometimes works on the first try, but many people need more than 1 round of IVF to get pregnant. IVF definitely increases your chances of pregnancy if you’re having fertility problems, but there’s no guarantee — everyone’s body is different and IVF won’t work for everyone. |
|
| |
| What’s the IVF process? |
| |
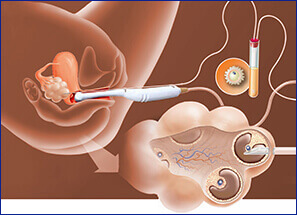
The first step in IVF is taking fertility medications for several months to help your ovaries produce several eggs that are mature and ready for fertilization. This is called ovulation induction. You may get regular ultrasounds or blood tests to measure your hormone levels and keep track of your egg production.
Once your ovaries have produced enough mature eggs, your doctor removes the eggs from your body (this is called egg retrieval). Egg retrieval is a minor surgical procedure that’s done at your doctor’s office or at a fertility clinic.
You’ll get medicine to help you be relaxed and comfortable during the procedure. Using an ultrasound to see inside your body, the doctor puts a thin, hollow tube through your vagina and into the ovary and follicles that hold your eggs. The needle is connected to a suction device that gently pulls the eggs out of each follicle. |
|
 |
| |
 |
|
In a lab, your eggs are mixed with sperm cells from your partner or a donor — this is called insemination. The eggs and sperm are stored together in a special container, and fertilization happens. For sperm that have lower motility (don’t swim as well), they may be injected directly into the eggs to promote fertilization. As the cells in the fertilized eggs divide and become embryos, people who work at the lab monitor the progress.
About 3-5 days after the egg retrieval, 1 or more embryos are put into your uterus (this is called embryo transfer). The doctor slides a thin tube through your cervix into your uterus, and inserts the embryo directly into your uterus through the tube.
Pregnancy happens if any of the embryos attach to the lining of your uterus. Embryo transfer is done at your doctor’s office or at a fertility clinic, and it’s usually not painful. |
|
Plan on resting for the rest of the day after your embryo transfer. You can go back to your normal activities the next day. You may also take pills or get daily shots of a hormone called progesterone for the first 8-10 weeks after the embryo transfer. The hormones make it easier for the embryo to survive in your uterus. |
| |
| What are the side effects of IVF? |
| |
Like all medications and medical procedures, IVF has some risks and possible side effects. These include:
Your doctor can talk with you about any questions or concerns you have about IVF risks and side effects.
IVF can also be difficult emotionally, both for the person having the procedures and for their partner and/or family. Many people doing IVF treatments struggle with depression and anxiety throughout the process.
Talking with people who’ve been through fertility struggles and IVF can be really helpful if you’re feeling overwhelmed or discouraged. Online and in-person communities are also good places to meet people who understand what you’re going through and can offer advice and support. Counselors and therapists can also be sources of comfort. |
| |
| |
|
| IRREGULAR PERIOD |
| |
| The normal length of a woman's menstrual cycle is 28 days, but this varies between individuals. Irregular menstruation is when the length of the cycle is more than 35 days, or if the duration varies. |
| |
A period, or menstruation, is the part of the menstrual cycle in which the endometrium, which is the lining of the uterus, is shed. This appears as bleeding from the womb that is released through the vagina.
Periods usually start during puberty, between the ages of 10 and 16 years, and they continue until menopause, when a woman is 45- to 55-years old.
Irregular periods, also called oligomenorrhea, can occur if there is a change in contraception method, a hormone imbalance, hormonal changes around the time of the menopause, and endurance exercises.
Treatment for irregular periods during puberty and around the menopause is not usually necessary, but if irregular periods occur during the reproductive years, medical advice may be necessary. |
|
 |
| |
| Symptoms |
| |
 |
|
A menstrual cycle lasts around 28 days, but it can vary from 24 days to 35 days, depending on the individual.
Most women have between 11 and 13 menstrual periods each year. Bleeding usually lasts around 5 days, but this too can vary, from 2 to 7 days.
When menstruation first starts, it can take up to 2 years to establish a regular cycle. After puberty, most women's menstruation is regular. The length of time between each period is similar.
However, for some women, the time between periods and the amount of blood shed vary considerably. This is known as irregular menstruation.
|
|
| |
The main symptom of irregular menstruation is when the cycle is longer than 35 days, or if it varies in length.
If there are changes in blood flow, or if clots appear that are more than 2.5 centimeters in diameter, this is also considered irregular. |
|
 |
| |
| Causes |
| |
| A number of factors increase the chance of irregular menstruation. Most relate to hormone production. The two hormones that impact menstruation are estrogen and progesterone. These are the hormones that regulate the cycle. |
| |
| Hormonal influences |
| |
 |
|
Life cycle changes that influence the hormonal balance include puberty, menopause, pregnancy, and childbirth, and breastfeeding.
During puberty, the body undergoes major changes. It can take several years for the estrogen and progesterone to reach a balance, and irregular periods are common at this time.
Before menopause, women often have irregular periods, and the amount of blood shed may vary. Menopause occurs when 12 months have passed since the woman's last menstrual period. After the menopause, a woman will no longer have periods.
During pregnancy, menstruation ceases, and most women do not have periods while they are breast-feeding. |
|
| |
Contraceptives can cause irregular bleeding. An intrauterine device (IUD) may cause heavy bleeding, while the contraceptive pill can cause spotting between periods.
When a woman first uses the contraceptive pill, she may experience small bleeds that are generally shorter and lighter than normal periods. These usually go away after a few months.
 Other changes that are associated with irregular periods include: Other changes that are associated with irregular periods include:
- extreme weight loss
- extreme weight gain
- emotional stress
- eating disorders, such as anorexia or bulimia
- endurance exercise, for example, marathon running.
A number of disorders are also linked to missed or irregular menstruation. |
| |
| Treatment |
| |
 |
|
Treatment, if needed, will depend on the cause.
Puberty and menopause: Irregular periods that occur during puberty or as the woman approaches menopause do not usually need treatment.
Birth control: If irregular bleeding is due to contraception, and it continues for several months, the woman should talk to a health care professional about other options.
PCOS and obesity: In cases of PCOS, overweight, or obesity losing weight may help stabilize menstruation. A lower weight means the body does |
|
not need to produce so much insulin. This leads to lower testosterone levels and a better chance of ovulating.
Thyroid problems: Treatment for the underlying problem is likely to be prescribed. This may include medication, radioactive iodine therapy or surgery.
Stress and eating disorders: Psychological therapy may help if emotional stress, an eating disorder, or sudden weight loss have triggered irregular periods. This may include relaxation techniques, stress management, and talking to a therapist. |
|








 bloating
bloating
