
Dr. Sankar Dasmahapatra
Uterine Fibroids Specialist in Kolkata, India
DGO, MS, Fellowship in Gynaecological Lap Surgery (Sydney -Australia)
Consultant Gynaecologist & Obstetrician
Infertility Specialist & Lapaoscopic Surgeon
DGO, MS, Fellowship in Gynaecological Lap Surgery (Sydney -Australia)
Consultant Gynaecologist & Obstetrician
Infertility Specialist & Lapaoscopic Surgeon
Uterine fibroids are benign (noncancerous) masses of muscle tissue that enlarge and/or distort the uterus and sometimes the cervix. Fibroids originate from the smooth muscle cells within the myometrium or wall of the uterus. In most cases there are multiple fibroids, but occasionally a single fibroid may occur. Other terms for uterine fibroids are myomas or leiomyoma.
It is estimated that uterine fibroids occur in one out of every four to five American women. African American women are over three times more likely to develop fibroids than Caucasian women. Usually, fibroids develop when a woman is in her 30s or 40s, and become smaller after menopause. Most fibroids do not require treatment. However, they may cause excessive uterine bleeding, pain, abnormal pressure sensations, and, less commonly, infertility, miscarriage, and premature delivery. Removing the fibroids surgically can usually correct these problems. However, there is a chance that additional fibroids and/or postoperative scarring will occur.

Cause
Increased Estrogen Levels
The exact cause of uterine fibroids is unclear, but there is evidence suggesting that they require estrogen for growth. For example, fibroids some times grow larger during pregnancy when the body produces more estrogen.
During menopause when estrogen levels decline, fibroid growth generally subsides. Consequently, fibroids rarely require treatment after menopause.
Types of Fibroids
Fibroids are usually found in or around the uterus, but they sometimes occur in the cervix. Fibroids can be divided into three categories: subserous, intramural, or submucous. Subserous fibroids are located in the outer wall of the uterus. Intramural fibroids are found in the muscular layers of the uterine wall, and submucous fibroids are located on the inner wall of the uterus and may protrude into the cavity. About 55 percent of fibroids are subserosal; 40 percent are intramural; and 5 percent are submucosal.
Symptoms-
Many women with uterine fibroids have no symptoms. However, approximately one-third report abnormal uterine bleeding, a feeling of pressure or pain in the pelvic or lower abdomen, or the presence of a mass. As fibroids enlarge and grow, the mass can become very large. Some women notice that their abdomen is larger and their clothes are tighter. Others can feel something protruding from the lower abdomen.
1) Abnormal Uterine Bleeding
Abnormal uterine bleeding is most common symptom associated with fibroids and is present in one-third to one-half of women undergoing fibroid-related surgery. Large fibroids can distort or enlarge the uterine cavity, and this creates a larger surface area for menstrual bleeding. Fibroids also put pressure on the endometrium and cause excessive bleeding. Because abnormal uterine bleeding can result from other causes, such as endometrial cancer and hormonal problems, it is important that women experiencing abnormal vaginal bleeding receive a thorough evaluation, even if uterine fibroids are present.
2) Pain
When a fibroid begins to grow rapidly, it may outgrow its blood supply and degenerate or decay, causing a painful, cramping sensation. This most often happens during pregnancy. When sudden, severe pain occurs, it can sometimes be caused by decaying, inflamed, or twisting fibroids. Large and bulky uterine fibroids may make intercourse painful.
3) Pressure Symptoms
Large fibroids may produce pressure on various pelvic organs such as the bladder, ureters, and rectum. Consequently, urinary frequency or urgency may occur because of decreased bladder capacity. Continued compression of these organs can also cause kidney damage if the fibroids are not removed. Fibroids in the lower uterus may put pressure on the large bowel and rectum, which could result in difficult bowel movements, constipation, or hemorrhoids.
4) Fibroids and Infertility
Fibroids may contribute to an infertility problem. Most often, submucosal or intramural fibroids inside the uterus are associated with infertility. However, only 2 to 3 percent of infertile women are unable to conceive due to uterine fibroids. Because of this, women and their partners should have a thorough infertility investigation to identify additional causes of fertility problems.
Infertility may result from uterine fibroids for several reasons. Changes in the endometrium may make it unlikely for a fertilized egg to attach to the uterine wall. In addition, one or both fallopian tubes may be compressed or blocked, thus preventing the sperm from reaching the egg. Conception rates after any of the surgical techniques (myomectomy) used to remove fibroids are generally good but depend upon other factors that influence fertility such as age, previous pregnancy, ovulatory status, the status of the fallopian tubes, and the male’s semen quality. Fibroids may increase miscarriage rates by impairing successful implantation of an embryo. Changes in the endometrium or in the blood supply to the uterus may also cause early miscarriage. In addition, increased risk of premature delivery and other pregnancy related problems can be associated with fibroids.
5) Cancer and Fibroids
The risk of fibroids being malignant is approximately 0.2 percent. This cancer is called leiomyosarcoma and is more likely to occur in a postmenopausal woman. However, if a fibroids begins to grow very rapidly, this may suggest that it has become cancerous and requires careful evaluation and potential removal of the uterus (hysterectomy).
6) Diagnosis
Uterine fibroids can usually be diagnosed during a pelvic examination. However, because other conditions such as ovarian tumors, bowel masses, and early pregnancy can be mistaken for fibroids, it will probably be necessary to undergo other tests. Several diagnostic procedures are available to determine the presence of fibroids.
7) Ultrasound
Ultrasound, either abdominal or vagina, is a procedure that uses sound waves to create a picture of the pelvic organs. The physician can look at an ultrasound picture to see if fibroids are present. Often, as fibroids vary in size, both transvaginal and transabdominal ultrasound is necessary to visualize them accurately.
8) Diagnostic Laparoscopy
Diagnostic laparoscopy can help the physician make a definitive diagnosis and can sometimes be used to remove fibroids. During this procedure, the physician will insert a slender, telescope-like instrument called a laparoscope into the abdominal cavity through a small incision near the navel. The laparoscope is used to look for abnormalities of the internal pelvic organs. This surgery is usually performed on an outpatient basis under general anesthesia and requires one to four days of recovery time. Diagnostic hysteroscopy is sometimes performed at the same time. In a few cases, fibroids can be removed during laparoscopy. This procedure is described later in this booklet.
9) Diagnostic Hysteroscopy
Diagnostic hysteroscopy is useful to determine the presence of submucous fibroids. This procedure involves the insertion of telescope-like instrument called a hysteroscopy through the vagina and cervix into the uterine cavity to look for abnormalities within the uterine cavity. The surgery can be done under local or general anesthesia. Sometimes the fibroids can be removed through the hysteroscope, but only in the operating room. This procedure is described later in this booklet.
10) Sonohysterography
With sonohysterography, a small catheter is placed inside the uterus to instill 15-20 cc of fluid during an ultrasound. This improves the physician’s ability to identify submucous fibroids which protrude into or distort the uterine cavity.
11) Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) produces a picture by absorbing energy from specific, high-frequency radio waves which can determine if fibroids are present. The created image can define the size and location of the fibroids and can help determine whether or not the fibroids are distorting the uterine cavity. Although MRI is very accurate, it is rarely needed to diagnose the presence of fibroids.
Treatment
Periodic Examinations
Most of the time, fibroids don’t require treatment. If a woman is not experiencing pain, a pressure sensation, infertility, or excessive bleeding, periodic examinations are generally sufficient to find out if there is a significant change in the fibroid size. This is especially true if she is planning a future pregnancy, when fibroids can grow and affect the pregnancy, or if approaching menopause, when fibroids generally shrink. Even if a woman is infertile, the presence of uterine fibroids is often only coincidental. Surgery to remove the fibroids should be considered only after a through evaluation of other factors which could be causing infertility. In fact, surgery on fibroids can sometimes make the infertility problem worse by creating pelvic adhesions (scar tissue).
Surgical Management of Fibroids
1) Myomectomy (Surgical Removal of Fibroids)Fibroids that are large enough to cause significant symptoms or rapidly growing fibroids may require surgery. Removal of only the fibroids, rather than the entire uterus, is called a myomectomy. Myomectomy is most often performed when the woman desires a future pregnancy or when she wishes to retain her uterus. Today, there are several options available for this surgery. In most cases, the size and location of the fibroids will determine the appropriate surgical technique. Small fibroids may be removed through less invasive hysteroscopy or laparoscopy procedures, but large, multiple, or inaccessible fibroids usually require laparotomy for removal. During a laparotomy, the physician will make an incision in the abdominal wall to remove the fibroids from the uterus. It usually takes about four to six weeks for a complete recovery. After a patient has undergone this surgery, a cesarean section may be needed for delivery because the muscular wall of the uterus may be weakened by the removal of many or large fibroids. The physician can make this determination at surgery.
The two major concerns with performing a myomectomy are minimizing blood loss and preventing surgically induced adhesions (scar tissue) that may impair future fertility. In rare cases, uncontrolled bleeding may require a hysterectomy. Sometimes women bank their own blood several weeks before myomectomy in case they might need a blood transfusion. If a woman and her physician decide that myomectomy is the best option, there are other risk factors that will need to be discussed. There is a chance that fibroids will reoccur and require further surgery. Pelvic adhesions may form which can impair fertility by affecting the tubes or ovaries. A laparoscopy can be used to evaluate any postoperative adhesions.
2) Operative Hysteroscopy
Small submucous fibroids located within the uterine cavity may be removed with operative hysteroscopy. During this procedure, the physician will insert a hysteroscope through the cervix into the uterus. Surgical instruments are then inserted through a channel in the hysteroscope to remove fibroids located within the uterine cavity. Generally, women can return to their normal activities within two days after operative hysteroscopy, and complications are rare.
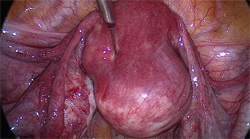
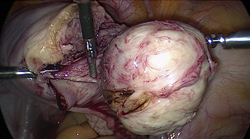
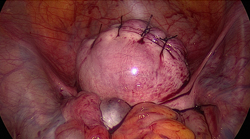
3) Operative Laparoscopy
In some cases, operative laparoscopy may be used to remove the fibroids if they are located on the outside wall of the uterus. During operative laparoscopy, the physician places a laparoscope into the abdomen through a small incision near the navel and then uses surgical instruments to remove the fibroids. Recovery time is usually two to seven days. A new techmique, called myolysis, in which the fibroid is at least partially, if not completely, destroyed by electrosurgery or other means is being developed.
4) Hysterectomy
If a woman has large fibroids that are symptomatic, and pregnancy is not desired, a hysterectomy or surgical removal of the uterus may be recommended. A vaginal hysterectomy, which removes the uterus through the vagina, or an abdominal hysterectomy, which requires a laparotomy, may be necessary. Recovery time is usually two to six weeks.
5) Medical Management of Fibroids:
GnRH analogs can be used to temporarily reduce the size of fibroids. GnRH analogs decrease estrogen levels by stopping the signal from the brain that sends a message to the ovaries to produce estrogen. This can significantly reduce the size of the fibroids. However, when GnRH analog therapy is discontinued, the fibroids usually return to their pretratment size within three to six months. GnRH analogs produce menopausal-like side effects such as hot flashes, vaginal dryness, mood swings, and sometimes bone loss. These medications cannot be used for extended periods of time unless special precautions are taken to prevent bone loss. Primarily, they are used before surgery to reduce uterine fibroid size. In women who have experienced excessive menstrual bleeding and have become anemic, GnRH anlogs may decrease vaginal bleeding. This medication, in combination with iron supplements, may improve anemia, allowing for the possibility of banking blood prior to surgery or reducing the need for a transfusion.
6) Psychological Aspects:
Women who have uterine fibroids may experience many different feelings. Some women say they feel defective because the condition involves their reproductive organs. It is important to remember that there are many more aspects to femininity and womanhood than one specific body part. Women who have experienced a miscarriage because of fibroids may feel guilty or anxious about future pregnancies. If a woman is faced with the possibility of losing her uterus, she may feel angry and sad, especially if future pregnancy is desired. It is important for a woman to discuss these feeling with her physician so that alternatives to hysterectomy can be discussed and considered. It is also helpful to seek support from family, friends, and support groups.
Summary
Uterine fibroids are benign masses of smooth muscle tissue in or around the uterine wall. They are commonly found in women during their reproductive years. Fibroids are usually harmless. However, some women experience abnormal uterine bleeding, pain, pressure, miscarriages, or infertility because of fibroids. There is also an extremely small chance that fibroids can develop into cancer. Therefore, it is important that a woman see her doctor at regular intervals to decide if she should undergo surgical removal of the fibroids or have a hysterectomy.